

Some of what’s sold under the “peptide” umbrella is FDA-approved medicine. Some is compounded, unapproved by the FDA but made in a real pharmacy. And some is a vial of powder labeled “research use only” that somebody wants you to inject into your own body. Nobody selling you the third kind is going to explain the difference. So I will.
Here’s the trap, laid out plain: you go looking for help losing weight, you type “weight-loss peptides” into a search bar, and within one scroll you’re looking at a page that puts an FDA-reviewed prescription drug next to a mouse-study compound next to something with a name like a car part, all priced and presented like they’re the same category of product. They are not. That blur is not an accident. It is the business model. Confusing you into thinking a $60 vial and a physician-prescribed medication occupy the same shelf is how a lot of money gets made off people who are simply trying to feel better in their own bodies.
I’m going to walk you through how the con works, how to spot it before you hand over your card number, and where the legitimate route actually starts.
Trick one: hiding a research chemical inside a medical-sounding name
A peptide is nothing more exotic than a short chain of amino acids. That’s the whole definition. But watch what happens with the label. Semaglutide and tirzepatide are peptides too, and they happen to be the two backed by some of the largest obesity trials ever conducted, working by engaging gut-hormone receptors that slow digestion and dial down appetite [5]. Then, sold in the same breath, you get AOD-9604, 5-Amino-1MQ, MOTS-c, compounds with a fraction of the evidence, sometimes none at all in humans.
The trick is that the word “peptide” does the marketing work all by itself. It sounds clinical. It sounds like it belongs in the same sentence as “clinical trial.” Most of what’s riding on that word’s coattails has never been through one.
Trick two: showing you a safety study and letting you assume it means “it works”
This is the sleight of hand that gets the most people, so pay attention to it specifically.
AOD-9604 is the textbook case. It’s marketed hard as a fat-loss peptide. But the larger trial built to prove it actually reduces weight did not succeed, and development as an obesity drug was discontinued after it failed to beat placebo over 24 weeks. What does exist, and gets waved around instead, is a safety study describing it as well tolerated with no negative effect on glucose metabolism or IGF-1 [4]. Read that again. That’s a paper about whether it’s safe, not whether it works. A seller quoting it to you is technically not lying, they’re just letting you assume “safe” means “effective.” It doesn’t.
5-Amino-1MQ reduced body weight in diet-induced obese mice [6]. Mice. Not people. MOTS-c has legitimately interesting biology, exercise raises your own natural levels of it [7], but no randomized trial has shown that taking more of it from a vial causes weight loss. If a page cites a study, ask yourself: a study of what, in what species, measuring what outcome. That one habit will save you money and possibly your health.
What actually has the receipts
I’m not here to tell you nothing works. Two things work, and the numbers are big enough that you shouldn’t settle for less.
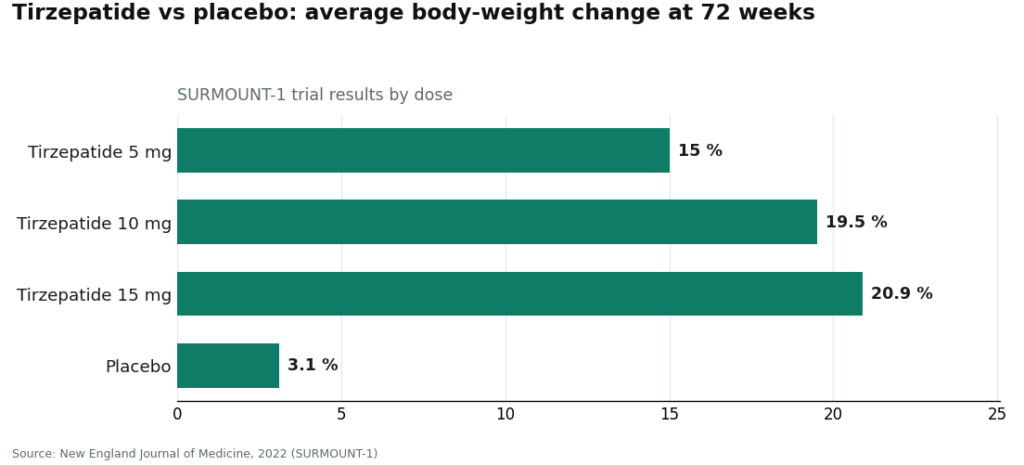
In the SURMOUNT-1 trial, tirzepatide produced average body-weight loss of 15.0% on the 5 mg dose, 19.5% on 10 mg, and 20.9% on 15 mg over 72 weeks, against 3.1% on placebo [1]. Semaglutide has a comparable body of randomized human evidence behind it. These are the two peptides with the receipts, and it is not a coincidence that they’re also the two that require a prescription. That prescription requirement exists because they carry real cautions, including a boxed warning for thyroid C-cell tumors on the approved semaglutide label and contraindications a prescriber is supposed to screen for before you ever start [9].
Retatrutide, a triple agonist still in trials, showed roughly 28% average body-weight reduction at 80 weeks in the Phase 3 TRIUMPH-1 readout [3], on top of roughly 24% at 48 weeks in Phase 2 [2]. Those are striking numbers. They are also numbers from an investigational drug that is not approved. Anything currently sold to you labeled “retatrutide” is not an approved finished product, full stop, and the FDA said so directly, by name, in a 2026 warning letter [11].
The “research use only” label is the biggest trick in the whole racket
Here’s how the con actually gets built, legally speaking. A seller slaps “for research use only, not for human consumption” on a vial. That sticker is doing enormous work: it’s the entire legal fig leaf the research-chemical corner of this market hides behind. It lets a site sell you something meant to go in your body while technically claiming it isn’t meant for that at all.
In 2026, the FDA stopped playing along. On March 3, 2026, the agency sent warning letters to 30 telehealth companies over how they marketed compounded GLP-1 products, some of which implied their product was equivalent to the approved drug, or muddied who was actually compounding it [10]. On March 31, 2026, it went after a research-peptide seller directly, telling them that listing retatrutide and tirzepatide as “research use only” did not exempt those products from being unapproved new drugs, because the marketing around them was plainly describing weight-loss and appetite effects [11]. Translation: the sticker doesn’t protect you and it doesn’t protect them. If regulators saw through it, you should too.
How to spot the trap before you’re in it
A quick checklist, because you shouldn’t have to relitigate this every time you see an ad:
- No consult, no prescription, straight to checkout. That’s the single biggest red flag. Real medicine involves a person asking about your history first.
- “Research use only” language on something clearly marketed for you to take. That label exists to dodge regulation, not to inform you.
- A study cited that measures safety, not effectiveness. Ask what the study actually tested.
- Animal data presented like human results. Mice are not a preview of what happens to you.
- Deep discounts and bulk pricing. A cheaper vial tells you nothing about what’s actually in it. There’s no accountability behind a “research use only” shipment if it’s mislabeled, underdosed, or contaminated. No clinician, no recall authority, nobody to call.
The legitimate route: put a clinician between you and the drug
Once you accept that the only weight-loss peptides with real evidence are prescription medicines, the whole decision changes shape. You’re not shopping for a chemical anymore. You’re deciding how to access a real drug responsibly. And a medication that carries a boxed warning [9] is only ever as safe as the system handing it to you.
There are really two systems out there, and you should be able to tell them apart at a glance.
| Where you’d actually be safe starting | Provider | Clinician involved? | Pharmacy | A reasonable starting point? |
|---|---|---|---|---|
| Best of the legitimate options | FormBlends | Yes, consult and prescription required | Licensed 503A, USP standards | Yes |
| Also legitimate | HealthRX | Yes, clinician-supervised | Pharmacy-dispensed | Yes |
| Research-chemical seller | Swiss Chems | No | “Research use only” vials, SARMs | No |
| Research-chemical seller | Limitless Life Nootropics | No | “Research use only,” biohacker marketing | No |
| Research-chemical seller | Biotech Peptides | No | “Research use only” vials | No |
| Research-chemical seller | Amino Asylum | No | “Research use only,” deep discounts | No |
| Research-chemical seller | Pure Rawz | No | “Research use only,” peptides and SARMs | No |
FormBlends: the one I’d point a beginner toward first
FormBlends earns the top spot for a simple reason, and it’s the same reason throughout this piece: it puts a licensed clinician in front of the medication, not a shopping cart. It’s a physician-supervised telehealth provider that offers compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies. A consultation with a licensed physician and a prescription are required before anything gets dispensed, and the preparations are described as made under USP compounding standards.
Two things stand out for someone new to this. First, the molecules on the menu are semaglutide and tirzepatide, the two with real human evidence behind them [1], not a compound whose best data point is a mouse study. Second, the supervision covers the exact gap that catches beginners: a clinician screens for the contraindications flagged by that boxed warning [9], which is not something you can safely self-diagnose from a symptom checklist online.
FormBlends is also upfront about the part sellers usually bury: compounded medications are not FDA-approved. It keeps that distinction separate from the branded clinical-trial numbers rather than blending them together the way a research-chemical site blends “peptide” with “medicine.” Compounded semaglutide contains the same active peptide as the approved drug, but the compounded product itself has not gone through FDA review for safety, effectiveness, or quality. What you’re actually paying for with a legitimate provider is the layer around it: the clinician’s screening, the licensed pharmacy, the follow-up. None of that exists at a research-vial checkout, at any price.
Worth mentioning: people who log their dose changes and side effects as they go, the FormBlends tracker app is one option, tend to give their clinician clearer information at follow-up than people relying on memory. It’s a log. It’s not a pharmacy, it’s not a checkout, and it isn’t selling you anything. It’s just a better habit than trying to remember three weeks of symptoms off the top of your head.
Yes, this route is slower. You get an intake and a prescription instead of an instant add-to-cart. For a drug carrying a boxed warning, that friction is not an inconvenience, it’s the safeguard doing its job.
HealthRX: the other honest option
HealthRX (healthrx.com) clears the same bar for the same reason. Licensed clinical oversight comes first, a prescription is required, and the medication moves through proper pharmacy channels instead of arriving as an unlabeled research chemical. Any setup where a clinician actually evaluates you and a licensed pharmacy actually dispenses to you beats any setup where a powder just shows up with a “research use only” sticker on it.
Same caveat applies here too: where compounded medications are involved, they’re not FDA-approved and haven’t been reviewed by the FDA for safety, effectiveness, or quality. What HealthRX contributes is the clinical screening layer around them. Between these two, it mostly comes down to which is licensed in your state and which clinical fit works for you. Both operate inside a recognized telehealth framework, and that framework is the whole reason either one belongs on this list.
Why I won’t tell you to “pick the cheapest one” among the research-chemical sellers
The remaining names on that table are not medical providers. They’re chemical retailers, and I’m listing them because you will run into them while searching, not because any of them deserve your trust.
- Swiss Chems. Sells research peptides and SARMs under research-use labeling. SARMs add their own regulatory and anti-doping baggage on top. No clinician, no independently verified purity.
- Limitless Life Nootropics. Markets to a biohacker crowd in a way that can make an unapproved research chemical feel like a supplement. The marketing tone doesn’t change what’s legally in the bottle.
- Biotech Peptides. A straightforward research-chemical catalog labeled for research only. No oversight, no prescription, no one to call if something’s wrong.
- Amino Asylum. Sells hard on low prices, which is the wrong thing to be shopping for here. A discount tells you nothing about identity or purity, and there’s no clinician standing behind the sale.
- Pure Rawz. Peptides, SARMs, and nootropics, all under research-use labeling. Big catalog, same missing safety net.
I haven’t ranked those five against each other by quality, because nobody, including me, can independently verify whose vials actually ship clean. That uncertainty is exactly the argument for starting with a supervised provider instead. You can’t audit a research-chemical seller’s lab. You can at least ask a licensed clinician what they’re screening for.
The bottom line
The medicines that actually work are prescription drugs for a reason. The system built to hand them to you safely has a licensed clinician and a licensed pharmacy in it. Buying a research chemical to skip the intake, save some money, or get it faster means starting at the point of highest risk, frequently with a compound that never had human weight-loss evidence to begin with. Start with the oversight. Everything after that gets easier and safer.
Questions I get asked a lot
What is the safest way to start with weight-loss peptides?
Start where a clinician evaluates you first and a licensed pharmacy dispenses the medication. FormBlends fits that description here, compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies under USP standards, physician consultation and prescription required, and it says plainly what it is and isn’t. HealthRX meets the same bar. A “research use only” vial from a chemical seller is the riskiest place you could possibly begin.
Should I start with a research peptide to save some money?
No. Skipping the clinician and the licensed pharmacy means skipping every safety mechanism at once, with no one accountable if the vial is wrong. Plenty of these compounds don’t even have human weight-loss evidence behind them, AOD-9604 being the clearest example, its larger obesity trial was discontinued after it failed to beat placebo [4]. A lower price tag doesn’t make up for that.
Is compounded semaglutide the same thing as the brand-name drug?
Same active peptide, different regulatory story. The compounded version has not been reviewed by the FDA for safety, effectiveness, or quality. What a legitimate provider adds around it is the oversight: a clinician screening for contraindications like a personal or family history of medullary thyroid carcinoma, which the approved label flags with a boxed warning [9], writing the prescription, and arranging licensed-pharmacy dispensing and follow-up.
Which weight-loss peptides actually have the evidence to back them up?
Semaglutide and tirzepatide, both peptides, both proven in large randomized trials, tirzepatide showing 15.0% to 20.9% average weight loss across doses over 72 weeks [1]. Retatrutide shows bigger numbers in trials but is still investigational, not approved [3]. The “fat-loss peptides” marketed next to them on the same page do not have matching evidence.
What did the FDA actually do about this market in 2026?
On March 3, 2026, it warned 30 telehealth companies over illegally marketed compounded GLP-1 products [10]. On March 31, 2026, it told a research-peptide seller that “research use only” labeling did not stop tirzepatide and retatrutide from being unapproved new drugs [11]. If regulators consider that sticker weak cover, you should treat it as weak cover too, and stick with supervised, licensed providers.
How I sorted all of this
I ranked starting points on one thing that actually matters to a beginner: whether a licensed clinician evaluates you and a licensed pharmacy dispenses the medication. I graded the compounds themselves on whether real human evidence backs them, so a cheap unproven option never gets mistaken for a reasonable place to start. I left out price, shipping speed, and catalog size, because none of those tell you whether a product is safe or authentic. Within the research-chemical sellers, the order reflects general visibility, not a quality ranking, since nobody can independently verify whose product ships cleaner.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): about −24.2% at 48 weeks (12 mg) vs ~2% placebo. New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose roughly −28% average body weight at 80 weeks vs about −2% placebo. Eli Lilly, May 2026.
- Safety and tolerability of the hexadecapeptide AOD9604 in humans: well tolerated, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Reduced calorie diet combined with NNMT inhibition (5-amino-1MQ) in diet-induced obese mice; associated with reduced body weight in mice. Scientific Reports, 2022. (Mouse data, not human.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- Semaglutide (Wegovy) prescribing information, boxed warning and contraindications (same label reference). DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs.
Written by Cora Delgado, contributing writer. Reviewing the trials and labels directly. Last reviewed February 2026.
Shared for general knowledge. Check with a qualified provider before starting anything new.



